Embed Size (px)
Citation preview

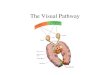
Week 3 Visual Pathway and
Visual field defects

Monocular retinal zone
Nerve fiber/optic nerve zone
Binocular chiasmal zone
Post chiasmal zone


Field defects are found opposite in the VF to the location of the damages in the eye.

RETINAL DETACHMENT VISUAL FIELD

Choroidal lesions care caused by tumors, inflammations, infection, or fluid leaks.
This type of damage does not respect the horizontal or vertical meridian.

EPI RETINAL MEMBRANE TEAR WITH BLEEDING HAMANGIOBLASTOMA

Damage may be caused by toxicity, inflammation, infections or heredity.

A diffuse pattern of field loss ( rod damage) forming a ring a variable scotomas that will expand outward toward the periphery and inward toward the fovea until blindness results.

Damage to cone receptors causing damage to the central 5 degrees.
Decreased color and VA will result.

Retinal layer Subretinal layer Rods and cones Retinitis pigmentosa Macular pathology
All defects will be monocular.
Most pathology will be visible with a scope.
Lesions temporal to the fovea will present nasal on VF.
Lesions can cross all meridians.
Central scotomas will cause abnormal VA and color vision.

Nerve fiber layer. Most common
cause is glaucoma. Also may be caused by trauma, blood vessel occlusions, infections, inflammations and tumors

(swelling of the disc)
Produces a field loss by pushing the surrounding retina out from the disc creating an enlarged blind spot.
It will present more concentric than an enlarged blind spot caused by glaucoma.

Macular and papillomacular defects create central or ceccocentral scotomas

Bjerrum area of nerve fiber layer.
15 degrees off fixation.
Defect in this area will cause an arcing VF loss opposite of the damage.
Will start small and increase in size over time.

Nerve fiber layer Optic nerve
(papilledema) Nerve fiber pattern
defects Bjerrum area
defects
All defects are monocular.
Defect will point to the disc since the nerve fibers are traveling toward this point.
All pathology will be visible with a scope

GLAUCOMATOUS DEFECTSDAMAGE TO NERVE FIBER LAYER WILL SHOW ON VF.

TEMPORAL WEDGE NASAL STEP

OPTIC NERVE CENTRAL SCOTOMA VISUAL FIELD


All will be monocular only effecting the damaged eye.
Damage to the nerve fiber layer will be caused by glaucoma.
The VF will show up opposite of the damaged area.
Specific areas of nerve fibers that have been damaged will respect the horizontal meridian and point in the direction of the disc.
Disc problems will be visible with a scope.


Caused by pituitary tumors or swelling,
Always bi temporal. Not visible with a
scope. CT scan or MRI needed
to show defect. Bilateral hemianopia
(temporal). Will respect vertical
meridian. Will start small and
gradually increase in size.
Bi temporal VF loss characteristics


LATERAL GENICULATE BODY OPTIC RADIATIONS

Not visible with a scope.
Problem will be visible with CT or MRI scan.
Homonymous defect will always be present. (Same side)
Will start out small and gradually get larger.
Will be hemianopic and will respect the vertical meridian.

Follow the pathway-
Page 22 in your text.
What is this problem?




See you next week for Goldmann Perimetry lecture.