Embed Size (px)
Citation preview

APOMORPHINE OLD DRUG ; NEW LIFE?
Dr Susan H Fox MRCP (UK), PhD Professor Neurology, University of Toronto
Movement Disorders Clinic, Toronto Western Hospital
CNSF, Halifax
June 25th 2018

DISCLOSURES Nature of relationship(s) Name of for-profit or not-
for-profit organization(s)
Description of relationship(s)
Any direct financial
payments including
receipt of honoraria
WPC; CHDI; AAN; MDS Honoraria for participation on
Committee/Conference
Speaker/Chair.
Membership on advisory
boards or speakers’
bureaus
Merz; Orion; Sunovion*;
Palidan*; Teva; Seqirus;
Zambon
Advisory board and Speaker
Funded grants or clinical
trials
Michael J Fox Foundation
for Parkinson Research;
Edmund J Safra
Foundation; Parkinson
Canada; NIH; CIHR.
Biotie; Cynapsus
(Sunovion)* ; Eisai; Kyowa
Funding for research
Site PI for Clinical Trials
* Companies developing Apomorphine products in Canada

Apomorphine
• Short-acting dopamine D2>D1 receptor agonist
• Derived from morphine; but no opioid properties

Clinical Uses
• Erectile dysfunction - first described by Ancient Egyptians (naturally occurring in blue lotus N. caerulea)
• Emetic – Alcoholism; ‘The Keeley Cure’ (1870s to 1900) contained apomorphine; animal medicine
• Parkinson's disease • Weil, 1884 • Schwab RS, Amador LV, Lettvin JY (1951). Apomorphine in Parkinson's
disease. Transactions of the American Neurological Association. 56: 251–3

Use of Apomorphine in PD
• Subcutaneous administration due to low oral bioavailability (first pass metabolism) – Intermittent injection
– Infusion
• Benefit in PD – Effective anti-parkinsonian action
– Intermittent s.c. injection provides rapid onset
– More reliable that oral levodopa (no GI issues) • Licensed for use in many countries (Available Europe since 1980s;
US 2004 ) as adjunct in advanced PD for treating OFF periods

Efficacy of intermittent subcutaneous injections of apomorphine shown in many
studies
– Rapid onset: mean onset in 6 to 14 minutes – Short duration: mean duration of effect is 36 to 61.9
minutes
• Overall decrease in daily 'off' time is - 2.6 to - 4 hours of the waking day
– Average dose of each injection = 2 – 6 mg
• Up to 3x per day
• Review of 21 studies, including 8 DBRCT (n=126), 6 crossover; 13 open-label studies (n=202). Chen J J, Obering C. Clinical Therapeutics 2005; 27(11): 1710-1724

Dose – dependent improvement in PD motor scores


Apomorphine : Side effects of drug
Orthostatic hypotension = 10% Reason to discontinue 2% Dose-related Initial and long-term Rx
Apomorphine; available in Canada Intermittent subcutaneous injections
Canada Jan 23rd 2018: The CADTH Canadian Drug Expert Committee (CDEC) recommended apomorphine hydrochloride (apomorphine) be reimbursed for the acute, intermittent treatment of hypomobility “off” episodes (“end-of-dose wearing off” and unpredictable “on/off” episodes) if the following criterion and conditions are met: Criterion: • Apomorphine should only be used as adjunctive therapy in patients who are
receiving optimized PD therapy (levodopa and derivatives and dopaminergic agonists) and still experiencing “off” episodes.
Conditions: • Patients treated with apomorphine should be under the care of a physician
with experience in the diagnosis and management of PD. • Reduction in price
– submitted unit price of $42.95 per 3 mL (30 mg) pen of apomorphine

Injectable Preloaded ‘Pen’
• Inject s.c. into lower abdomen or outer thigh
• Store at room temp; lasts 48 hours after first opening.
• Do not use if solution has turned green.
10mg/ml 3ml prefilled pen
Pictorial representation only

Practicalities: Initial dose finding
• Pre-treat with anti-emetic Domperidone 10mg TID for 3 days (- > 50% discontinue after 6-8 weeks )
• ECG (for QTc) (small dose related increased QTc if > 6mg used)
• In-clinic dose finding • Suggested method
– Omit morning PD meds ie. OFF and 1h post 10mg domperidone – Measure BP (lying and standing)
– Start with 1 mg or 2mg (- depending on BMI; risk of lowering BP)
• Assess benefit (ideally UPDRS part III) after 30 min and BP
– If no effect wait 1.5 hour post injections and repeat with 2 or 3mg – If no effect bring back a second day or wait 1.5 hour post injection and repeat
with 3 or 4 mg • (total daily dose of apomorphine HCl should not exceed 100mg and individual bolus
injections should not exceed 10 mg).

Practicalities: Long term use
• Requires patient (and physician education)
• Support for patient - ? Telephone
• Ideal – In clinic and home visit PD specialist Nurses?

Licensed: 23 countries; UK>25 years.
? Canada
Continuous subcutaneous apomorphine perfusion pump

Use of Apo Pump in PD
• Indication: Advanced PD with disabling motor fluctuations and dyskinesia
• Alternative to Levodopa-Carbidopa Gel Infusion (Duodopa) • Alternative to Deep brain stimulation surgery
• Open-label/un-controlled studies/Case series: • Reduces OFF time • Reduces dyskinesia, • Reduces L-dopa dosing
• Phase III DBRCT (abstract only)
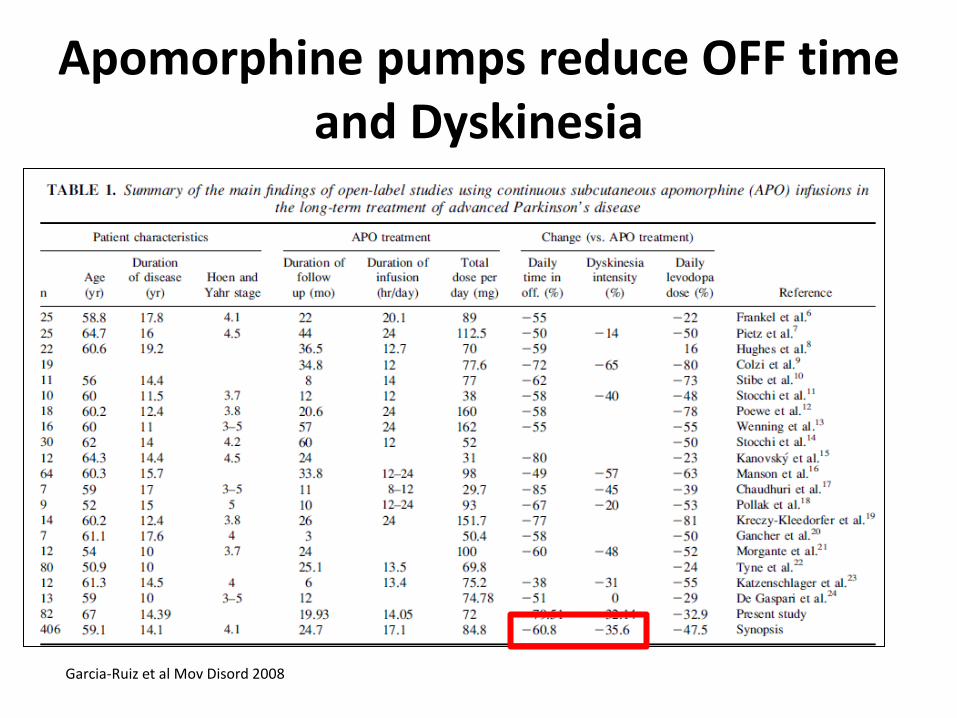
Apomorphine pumps reduce OFF time and Dyskinesia
Garcia-Ruiz et al Mov Disord 2008

52 week open-label phase
COMT, catechol-O-methyl transferase inhibitor, DA, dopamine agonists; MAO-B, monoamine oxidase-B inhibitor.
TOLEDO: randomized, double-blind, placebo-controlled Phase III study of subcutaneous apomorphine infusion in patients with Parkinson´s disease and motor fluctuations not well
controlled on optimized oral medical treatment Katzenschlager R, et al AAN Boston April 2017
107 patients in 23 centers, 7 countries
≥3 h OFF/day despite optimized treatment Slides courtesy of Dr Katzenschlager

Main results
APO (n=54) Placebo (n=53)
At least one treatment-emergent AE (TEAE) 50 (92.6%) 30 (56.6%)
Most common TEAE (≥10% of patients)
Skin nodules at infusion site
Nausea
Somnolence
Skin erythema at infusion site
Dyskinesia
Headache
Insomnia
24 (44.4%)
12 (22.2%)
12 (22.2%)
9 (16.7%)
8 (14.8%)
7 (13.0%)
6 (11.1%)
0
5 (9.4%)
2 (3.8%)
2 (3.8%)
0
2 (3.8%)
1 (1.9%)
Serious AEs 5 (9.3%) 2 (3.8%)
Safety and tolerability
ON time without troublesome dyskinesia: treatment
difference: 1·97 hours [95% CI: 0.69, 3.24; p=0.0008]
Primary endpoint: absolute change in OFF time from
baseline to Week 12 derived from patient diaries
OFF time treatment difference -1.89 hours (95% CI: -3.16, -0.62;
p=0.0025)
Patient Global Impression of Change:
Favored apomorphine (p<0.0001)
• Level 1 evidence:
• Significant, clinically meaningful reduction in OFF time,
• Significant increase in ON time without troublesome dyskinesia

Additional Side effects of Apo Pump
• Subcutaneous nodules (50%)
• Ultrasound reduces induration
• Rotation of injection
• Rare: Coombs positive Haemolytic anemia (6%) ;
• check complete blood count and hemolytic parameters q6 monthly
• Symptoms = pallor, dyspnea, jaundice

Intervention
ADD-ON THERAPY FOR MOTOR
FLUCTUATIONS
Efficacy conclusions Safety Implications for
clinical practice
Dopamine agonists Non-ergot
Pramipexole Efficacious Acceptable risk
Clinically useful
Pramipexole ER Efficacious Clinically useful
Ropinirole Efficacious Clinically useful
Ropinirole PR Efficacious Clinically useful
Rotigotine Efficacious Clinically useful
Apomorphine Intermittent s.c Efficacious Clinically useful
Apomorphine infusion Likely Efficacious Possibly Useful
Piribedil Insufficient evidence Investigational
Ergot Pergolide Efficacious Acceptable risk with
specialized monitoring
Clinically useful
Bromocriptine Likely Efficacious Possibly useful
Cabergoline Likely Efficacious Possibly useful
Levodopa/ peripheral decarboxylase inhibitor
Controlled release Insufficient evidence Investigational
Extended IPX066 Efficacious Clinically useful
Intestinal Infusion Efficacious Acceptable risk with
specialized monitoring Clinically useful
Other delivery strategies for apomorphine?
• Prior failures with
– Intravenous
– Nasal
– rectal
• local skin reactions • Acidic; pH 3.0 to 4.0
– Intravenous - crystallizes causing thrombosis

Sublingual apomorphine? tried before…………..
Montastruc et al Sublingual apomorphine: a new pharmacological approach in Parkinson's disease? J Neural Transm Suppl 1995;45:157-61. • “Sublingual apomorphine was shown to reduce extrapyramidal symptoms. • Sublingual apomorphine has the advantage of being easier to administer than subcutaneous
injection. …… For the moment, the long-term use of sublingual apomorphine is limited by two major problems: 1. Time for dissolution and switch "on" (which is longer than after subcutaneous route) 2. Local side effects (stomatitis). …….. • Further clinical studies using either more efficient (tablets with faster dissolution) and better
tolerated sublingual formulations ……….should be carried on before recommending this approach in the treatment of Parkinson's disease”.

Sublingual Apomorphine
• APL-130277: soluble, sublingual, strip formulation.
– Thin bilayer – apomorphine and optimising absorption ; second layer - buffer
• FDA granted APL-130277 fast track designation as a treatment for Parkinson’s off episodes – Aug 2016. New Drug Application for APL-130277 : filed with FDA March 2018. • Health Canada: in submission
• Drink water before using • Place on bottom of tongue • Don’t swallow for 2 mins

6/25/2018
• Open-label
– 20 PD subjects
• 78% subjects fully - ON at 30 mins

Open-label dose-titration study of APL-130277
N = 76 PD with early AM OFF and total daily OFF time ≥2 hours/day
• Titration sequence for APL-130277 was 10mg, 15mg, 20mg, 25mg, 30mg. • MDS-UPDRS Part III at 15, 30, 45, 60 and 90 minutes. Results » 83% of patients full ON with median dose 20mg.
• Mean Onset in 5-12 minutes. • 15 Min ON in 22 % • 30 Min ON in 59%
» At 30 and 90 minutes there was a 22 and 16-point improvement in the
MDS-UPDRS Part III, respectively.
R. Hauser, S. Isaacson, A. Espay, R. Pahwa, D. Truong, E. Pappert, P. Gardzinski, B. Dzyngel, A. Agro, H. Fernandez. Efficacy of sublingual apomorphine film (APL-130277) for the treatment of OFF episodes in patients with Parkinson’s disease: results from the Phase 3 study dose-titration phase [abstract]. Mov Disord. 2017; 32 (suppl 2).
Phase 3 APL-130277 for the Acute Treatment of OFF Episodes in Parkinson's Disease
(CTH 300) • 141 PD with motor fluctuations (total daily "OFF" time duration of ≥ 2 hours )
• APL-130277 (10 -35 mg) /placebo ; Two phases:-
1. In clinic open label dose titration: to determine dose at which patient achieved Full- ON: (22% discontinued; 8.5 % AE; 7% lack of benefit)
2. 12 week treatment phase: 109 subjects randomized to dose /placebo use of APL up to 5x /d (16% placebo v 37% APL discontinued)
Primary endpoint: MDS UPDRS III at 30 min post dose after 12 weeks Multiple secondary endpoints
• % subjects with Full ON at 12 w; CGI;PGI; UPDRS II (ADL); home diary rate of Full ON after dose 1- 2d prior to visit; PDQ36 (QAL); UPDRS III at 15 min
• Safety and tolerability
Olanow CW et al Poster 2nd Pan American Section of the International Parkinson and Movement Disorder Society meeting , Jun 23rd , 2018

Results • Significantly improved MDS-UPDRS Part III score at 30 minutes
(- 7.6 points v placebo) at Week 12 (P = 0.0002)
• 35% APL subjects full ON at 30 min v 16% placebo (P < 0.001) – Median time to onset of effect = 22 min (22% ON at 11 min)
• Home diary 79% APL full ON at 30 min v 31% placebo
Treatment-emergent adverse events in APL group (TEAEs led to withdrawals in 27% of APL v 9% in placebo)
• Nausea (27.0 %), • Somnolence (14.9 %), • Dizziness (14.2 %), (no significant OH) • Oral mucosal erythema 7.4% = glossodynia, lip edema, lip swelling,
oropharyngeal swelling, and throat irritation.
• CTH 301 NCT02542696 Long-term safety, efficacy (n = 226)

Comparison s.c. vs s.l apomorphine
Subcutaneous • Faster acting (onset 5-10 min) • More reliable effect (93% on)
• Side effects – Orthostatic hypotension can be significant; nodules
• Ease of use: assembling injections;
• Patient training/preference? • Cost?
Sublingual • Onset in 20 min • Variability in effect (31 - 78%
full on at 30 min)
• Side effects – less OH but oral mucosal reactions (idiosyncratic?)
• Ease of use: strip easier?
• Patient training/preference? • Cost?
Open-Label, Randomized, Crossover Trial to evaluate sublingual administered APL-130277 (apomorphine)
compared to subcutaneously administered apomorphine (NCT03391882)
Open-label, crossover titration subjects will be randomly assigned to APL-130277 or APO s.c. and titrated to the dose that turns them from the practically defined "OFF" state to the full "ON" state. Then crossed over to the other drug and similarly titrated to the dose that provides a full "ON" state.
• PD with motor fluctuations (n = 85)
• End point – Percentage of subjects preferring sublingual APL-130277
(apomorphine) compared to percentage of subjects preferring subcutaneous APO (apomorphine) at 3 months

Conclusions • Apomorphine is a short acting dopamine D1,2 receptor
agonist • Effective anti parkinsonian action
• Uses: Advanced PD for disabling off periods especially
sudden/unpredictable offs.
• Subcutaneous delivery • (sublingual – pending FDA/HC reviews)
• Side-effects : as per dopamine agonists plus subcutaneous
effects local effects.





























