Acute Respiratory Distress syndromeSophy sony, BMCON
DEFINIION ARDS is a severe lung disease caused by avariety of
direct and indirect issues. It is characterized by inflammation of
the lung parenchyma leading to impaired gas exchange with
concomitant systemic release of inflammatory mediators causing
inflammation, inflammation, hypoxemia and frequently resulting in
multiple organ failure. failure. This is often fatal, usually
requiring mechanical ventilation and admission to an intensive care
unit. A less severe form is called unit. acute lung injury (ALI).
ALI).
Aiso known as. Noncardiogenic pulmonary
edema;IncreasedIncreased-permeability pulmonary edema; Stiff lung;
Shock lung; ARDS; Acute lung injur
Historical Background Since WWI physicians have recognized a
syndrome ofrespiratory distress, diffuse lung infiltrates and
respiratory failure in pt with various medical conditions including
from battle trauma to severe sepsis, pancreatitis, massive
transfusions etc
In 1967, Ashbaugh et al become the first to describe thesyndrome
which they referred to as adult respiratory distress syndrome in 12
such patients (1)
Historical Background in 1971, Ashbaugh and Petty further
defined thesyndrome in a form that summarized the clinical features
well (but lacked specific criteria to identify pts systematically)
(2)
- severe dyspnea - cyanosis refractory to O2 - decreased pulm
compliance - diffuse alveolar infiltrates on CXR - atelectasis,
vascular congestion, hemorrhage, pulm edema and hyaline membranes
at autopsy
Historical Background in 1988, a more expanded definition was
proposed thatquantified the physiologic respiratory impairment
through the use of 4-point lung injury scoring system (3) 4- level
of PEEP - P/F RATIO - static lung compliance - degree of
infiltration on CXR - *also included nonpulm organ dysfunction This
definition still had its shortcomings in that it specific criteria
to r/o cardiogenic pulm edema and is not predictive of outcomes
Historical Background 1994 American - European Consensus
ConferenceCommittee (AECC) came up with definition that became
widely accepted syndrome from adult respiratory distress - Acute
onset - bilateral infiltrates on CXR - PCWP =< 18 mmHg - P/F
ratio =< 200 ( ALI if P/F ratio =< 300 )
also changed the name to acute respiratory distress defined it
as a spectrum of ALI
Epidemiology the problem has always been how to identify the
cases attempts at extrapolating incidences based on the
variousdefinitions offered above have resulted in various numbers
(1.5-8.3 (1.575/100,000) Scandinavia (reported incidence of
17.6/100,000 for ALI and 13.5/100,000 for ARDS (4) Washington
4/1999-7/2000) reported much higher numbers for
age4/1999ageadjusted incidence (5) - ALI - 86.2/100,000 person-yrs
(reaching 306 in ages 75-84) person75- estimated annually cases
base on these stats 190,600 - mortality 74, 500/yr
the first study using the 1994 AECC definition was done in
More recently the ARDSNet study (done in King County,
Morbidity and Mortality prior to ARDSNet study - mortality rate
for ARDS has been estimated at 40-70% 40ARDSNet found a much lower
overall mortality rate 30-40% (6) 30notable that MR increases with
age: 24 % ages 1515-19 and 60 % in > 85 yrs 2/2 co-morbid
conditions coMortality is attributable to sepsis or multiorgan
dysfunction
Morbidity and Mortality Morbidity- prolonged hospital course-
nosocomial courseinfections especially VAP - wt loss - muscle
weakness - functional impairment in months following
CausesDIRECT LUNG INJURY(primary lung injury)COMMON PNA
Aspiration LESS COMMON Pulm contusion Fat emboli Near-drowning Near
Inhalation injury Reperfusion pulmonary edema after CPbypass
INDIRECT LUNG INJURY(secondry) INJURY(secondry)COMMON Sepsis
Severe trauma with shock and multiple transfusions LESS COMMON
Cardiopulm bypass Acute pancreatitis Transfusions Drug overdose
Anaphylaxis DIC Nonpulmonary sys.diseases Severe head injury
Pathophysiology Diffuse alveolar damage Lung capillary damage
Inflammation/pulm edema* Resulting severe hypoxemia anddecreased
lung compliance
Pathophysiology ARDS
Injury to the alv .cap.memb release of imflm. mediators imflm.
Damaged type2 alv cell
Surfactant production alv. Cap.mem. alv. vascular permiability
narrowing & Alv.compliance & recoil obsrtn
BROCHOCOSTRICTION Atelectasis outward migration of bld.cells&
fld bld.cells& hyaline mem. formation mem. from capillaries
impairment in gas exchange ARDS pul.oedema
lung compliance
Pul.HTN
PathophysiologyOccurs in stages 1. Exudative ( Acute Phase) 2.
Proliferative 3. Fibrotic 4. Recovery
Exudative phase (Acute Phase)(1Phase)(17days) Alveolar-capillary
barrier is formed by Alveolarmicrovascular endothelium and alveolar
epithelium Under normal conditions epithelial barrier is much less
permeable than endothelium Epithelium is made up of type I and II
cells Type I cells are injured easily and Type II cells are more
resistant
Exudative Phase In ALI/ARDS damage to either oneoccurs,adherence
of neutrophils to vas.endothelium--vas.endothelium--resulting in
increased permeability of the barrier. Ie. Ie. Capilary
permiability. Engorgement of perivascular permiability. &
peribronchial interstitial space interstitial edema, fluid crosses
the alv. Epithelium alv. Influx of proteinproteinrich edema fluid
into the alveolar space intra pulmonary shunt as blood passing
through them can not be O2nated. WOB, dyspnoea. dyspnoea. Injury of
Type I cells results loss of epithelial integrity and fluid
extravasation (edema) Injury of Type II cells then impairs the
removal of the edema fluid
Exudative Phase Dysfunction of Type II cellsproduction and
turnover of surfactant to alveolar collapse Widespred atelectasis
lung complance, complance, compromised gas exchange, hypoxemia
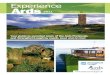
If severe injury to epithelium occurs
disorganized/insufficient epithelial repair occurs ie, ie,
hyaline membrane begins to line the alveoli resulting in fibrosis
and atelectasis. atelectasis. In addition to inflammatory process,
there is evidence that the coagulation system is also involved
pul.microvascular occlusion PA bld flow to ventilated portions dead
space, PulHTN
Exudative Phase
Proliferative Phase After acute phase, some pt will have
uncomplicated course and rapid resolution. Still may have
dyspnoea,tachypnoea, & hypoxemia. dyspnoea,tachypnoea,
Histologically first sigs of resolution are -initiation of lung
repair -organization of alveolar exudate -a shift from neutro to
lympho predominant pul. pul. Infiltrate. -Proliferation of type-2
pneumocyte along alv. typealv. Basement memb. & syn. of new
pul.surfactant memb. and differentiate into ty-1 pneumocytes. ty-
pneumocytes.
Proliferative/repertivePhase(7Proliferative/repertivePhase(7-21days)
With intervention (mechanical ventilation) there is clearance of
alveolar fluid Soluble proteins are removed by diffusion between
alveolar epithelial cells Influx of neutro., mono.,lympho., &
fibroblasts neutro., mono.,lympho., proliferation as a part of the
inflm. Response. inflm. Insoluble proteins are removed by
endocytosis and transcytosis through epithelial cells and
phagocytosis through macrophages Injured has immune regenerrative
capacity after a/c lung injury.
Proliferative Phase
Proliferative Phase Type II cells begin to differentiate into
Type Icells and reepithelialize denuded alveolar epithelium.
Further epithelialization leads to increased alveolar clearance
This phase is complete when the diseased lung is characterised by
-dense firouse tissue pul.VR & PHTN lung compliance(Bcos
interstitial fibrosis) compliance(Bcos Hypoxemia(due to thick
alv.mem diffusion limitation & shunting. *if repe. Phase
persists repe. widespread firosis,if arrested.leasion firosis,if
arrested.leasion resolves.
Fibrotic Phase (chronic/late) Intense inflammation leads to
obliteration of the normal lung architecture Occurs about 2-3 wks
after the initial injury. 2Alveolar space is filled with
mesenchymal cells and their products Reepithelialization and new
blood vessel formation occurs in disorganized manner Fibroblasts
also proliferate, collagen is deposited resulting in thickening of
interstitium Fibrosing alveolitis and cyst formation
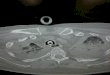
Fbrotic phase
Diffuse scaring & fibrosis
lung compliance + marked reduction in surface area bcos of
int.fibrosis hypoxemia PHTN from pul.vas. desruction & fibrosis
pul. pul. dead space . risk of pneumonia, morbidity
Consequences Impaired gas exhange leading to severehypoxemia -
2/2 ventilation-perfusion mismatch, ventilationincrease in
physiologic deadspace Decreased lung compliance due to the
stiffness of poorly or nonaerated lung Pulm HTN 25% of pts, due to
hypoxic vasoconstriction, Vascular compression by positive airway
compression, airway collapse and lung parenchymal destruction
Clinical Features Pts are critically ill develop rapidly
worsening tachypnea, dyspnea, tachypnea, dyspnea,hypoxia requiring
high conc of O2 Occurs within hours to days ( usually12-48
usually12hours) of inciting event Early clinical features reflects
precipitants of ARDS Physical exam shows cyanosis, tachycardia,
tachypnea and diffuse rales and other signs of inciting event
Clinical Features Initial presentation often insidious .
Initially may not experience res.sympts. res.sympts. Or only
cough,dyspnoea, tacypnoea, & restlessnes cough,dyspnoea,
tacypnoea, Chest aus.may be N or reveal fine scatterd crackles
ABG- mild hypoxemia, & res.alkalosis caused by
ABGhyperventilation.
Resp. alk. From hypoxemia&juxtra cap.receptors(+) alk.
cap.receptors(+) Cxr-N or evidance of minimal scattered
interstistial Cxrinfiltrates( on x-ray only after 30% in fld x-
c/f contd contd As ARDS progressesworsening of symptsbse of fld
accmln & lung compliance - WOB, tachypnea, I.C &
suprasternal retraction tachypnea, - PFT- lung compliance &
lung vol. esp FRC PFT- Tachycardia, diaphoresis, change in
sensorium with alt.mentation, alt.mentation, cyanosis , pallor -
O/A- scattered to diffuse crackles,rhonchi O/A- Cxr- diffuse
extensive B/L intestitial & alv infiltration, pl.effusion Cxr-
PAWP-does not PAWPas the cause is non cardiac - Hallmark of ARDS
hypoxemia, PaO2 / FiO2 5cm H2O Pao2 / Fio2 ratio < 2oo CHEST
Xray New B/L and alv.infiltrates PAWP 9-10gm% + Sa. O2 >/= 90%
Hb< 9-
Treatment Fluids ARDSNet study comparing a conservative and a
liberal fluid stategies (9) Rationale behind this study is
decreasing pulm edema by restricting fluids Randomized, using
explicit protocols applied for 7 days in 1000 pts in ALI
Randomization was into fluid liberal vs fluid conservative Primary
end point was death at 60 days Secondary end points included
vent-free days, ventorgan failure free days
Treatment Fluids Study did not show any significant difference
in 60 daymortality However pts treated with fluid conservative
strategy had an improved oxygenation index and lung injury score In
addition, there was an increased in vent-free days ventwithout
increase in nonpulm organ failures Also noted in this study is that
in fluid conservative group the fluid balance was more even than
negative which may indicate the observed benefit may be
underestimated
Treatment - VentilationGoals of ventilation in ARDS are to:
Maintain oxygenation by keeping O2 sats at 85-90% 85 Avoiding
oxygen toxicity and complication of mechanical ventilation
decreasing FiO2 to less than 65% within the 1st 24-48 hours 24-
Treatment - Ventilation Known TV in normal persons at rest is
667ml/kg But historically TV of 12-15ml/kg was 12recommended in
ALI/ARDS It was also recognized this strategy of high TV causes
Vent-associated lung injury as Ventearly as 1970s Then came the
land mark ARDSNet study which compared traditional TV to lower
TV
Treatment Ventilation ARDSNet ( low vs traditional TV) 861 pts
with ALI/ARDS at 10 centers Patients randomized to tidal volumes of
12mL /kg or 6 ml/kg (volume control, assist control) In group
receiving lower TV, plateau pressure cannot exceed 30 cm H2O 22%
reduction in mortality in patients receiving smaller tidal volume
Number-needed to treat: 12 patients Number-
ARDSNet PaCO2 Respiratory rate PaO2/F /FIO2 Plateau pressure
PEEP 6ml/kg 43 12 30 7 160 68 26 7 9.2 3.6 12m/kg 36 9 17 7 177 81
34 9 8.6 4.2
ARDSNet low vs traditional TV protocol * Calculated predicted
body weight(pbw)male: 50+2.3[height(inches)-60]
50+2.3[height(inches)female: 45.5+2.3[height(inches)-60]
45.5+2.3[height(inches)Mode: Volume assist-control assistChange
rate to adjust minute ventilation (not>35/min) PH goal 7.30-7.45
7.30Plateau press35/min) PH goal 7.30-7.45 7.30Plateau press