Embed Size (px)
Citation preview
DENTIGEROUS CYST
PREPARE BY ABU BAKAR SIDDIK city dental college Dhaka
INTRODUCTION A dentigerous cyst is one that results because of
the enlargement of the follicular space of the whole or part of the crown of an impacted or unerupted tooth and is attached to the neck of the tooth.
A dentigerous cyst encloses the crown of an unerupted tooth by expansion of its follicle and is attached to the neck of the tooth.
It is caused by alteration of reduced enamel epithelium after the completion of amelogenesis which results in fluid accumulation between epithelium and tooth crown.
HISTORY The term dentigerous cyst is a latin
word Denti means Tooth Gerous means Bearing or Producing In 1988 dentigerous cyst originated
from a female patient
DEFINATION OF CYST Cyst is defined as pathologic cavity or
sac within the hard or soft tissue that may contain
Fluid , semifluid or gas lined by epithelium, fibrous tissue or occasionally even by neoplastic tissue.
CLASSIFICATION INTRAOSSEOUS 1.Epithelial cyst A. Odontogenic epithelial origin- 1.Developmental a. Primordial cyst b. Dentigerous cyst c. Lateral periodontal cyst d. Calcifying odontogenic (Gorlin) cyst
2.INFLAMMATORY a. Radicular cyst (Apical/Lateral Periodontal) b. Residual cyst B. non-odontogenic epithelial origin 1.Fissural a. Median mandibular b. Median Palatal c. Globulomaxillary
2. Incisive canal cyst (nasopalatine duct or mediananterior maxillary) C.Non epithelial cyst-( pseudocyst) a. Solitary bony cyst b. Stafne’s bone cavity c. Anurysmal bone cyst D. Cysts of maxillary antrum a. Surgical ciliated cyst of maxilla B. Benign mucosal cyst of the maxillary antrum
SOFT TISSUE CYST A. Odontogenic- Gingival cyst: a. adult b. newborn B. Non odontogenic a. Anterior median lingual cyst b. Nasolabial cyst(Or nasoalveolar cyst) C. Retention cyst 1.salivary gland cyst- a. Mucocele b. Ranula
D. DevelopmentaL/congenital cyst’s a. Dermoid and epidermoid cyst b. Lymphoepithelial cyst c. Thyrogossal duct cyst d. Cystic hygroma E. Parasitic cyst’s a. Hydatid cyst’s b. Cysticcerocis
F. Heterotropic cyst’s: Oral cyst with gastric or intestinal
epithelium
DENTIGEROUS CYST Definition- An epithelial cyst containing fluid and one or
more imperfect teeth usually thought to result from defect in the enamel forming structure. OR ,An odontogenic cyst that surround the . crown of the imfacted tooth , caused by fluid accumulation between the reduce enamel epithelium and the enamel surface , resulting in a cyst in which the crown is located within the lumen
Dentigerous cyst : Enclose part or all of the crown of an
unerupted tooth develops from proliferation of the
reduced enamel epithelium Eruption cyst arises in an extra-alveolar
location
ORIGIN The exact histogenesis of dentigerous
cyst remain unknown ,but most authors favor a developmental origin from the tooth follicle

AETIOLOGY Develops by accumulation of fluid
between reduce enamel epithlium and crown after crown formation
By transformation of epithelium in the in the wall of dental follicle and uniting with the follicular epithelium
INCIDENCE
AGE: first to third decades SEX: equal in both sex SITE: maxilla -33%,mandible-67% most frequently located in angle of mandible . canine region of maxilla & mandible . maxillary 3rd molar area , rearly at anterior segment
CLINICAL FEATURE 1. It is aggressive type of cystic lesion but may
remain silent 2.usually painless , pain arise when secondary
infection occurs 3.If untreated-swelling became large 4.expanson of bone with subsequent facial
asymmerty 5.pus may discharge in case of secondary infection 6. In the region of cyst:- the tooth may remain
unerupted
CYSTIC CONTENTS1.Consist of clear yellowish fluid , in which cholesterol crystals may present 2. In case of long standing infection purulent p[us may present.
PathogenesisDentigerous cyst arise as a result of cystic change in the remnants of the enamel organ after enamel formation is complete . They enclose the crown of an unerupted tooth and are attached to the cementoenamel junction . They develop by expansion of the follicle when fluid collects or space is created between the reduced enamel epithelium surrounds a developing tooth and degenerates as a tooth is erupting . In the formation of as dentigerous cyst , fluid accumulation occurs when the erupting tooth compresses the tooth follicle and obstructs venous outflow which induces serum to cross through capillary walls .
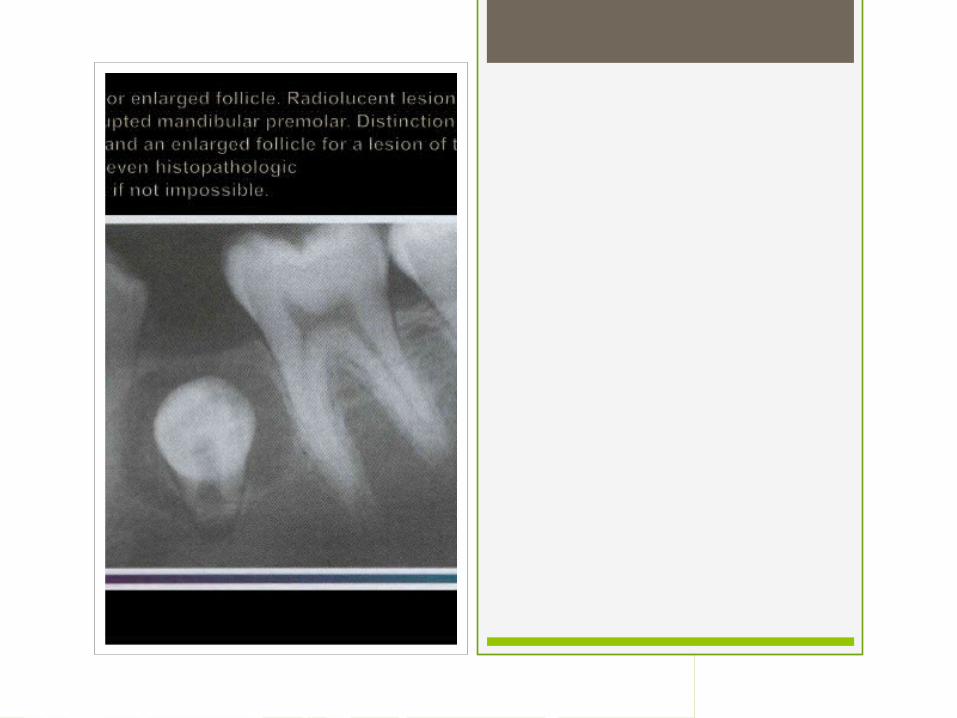
RADIOLOGICAL FEATURE 1.Welldefied radiolucent area 2.unilocular or mnultilocular radiolucency encircle
the crown of unerupted tooth 3.radiologically, the dental follicule may expand
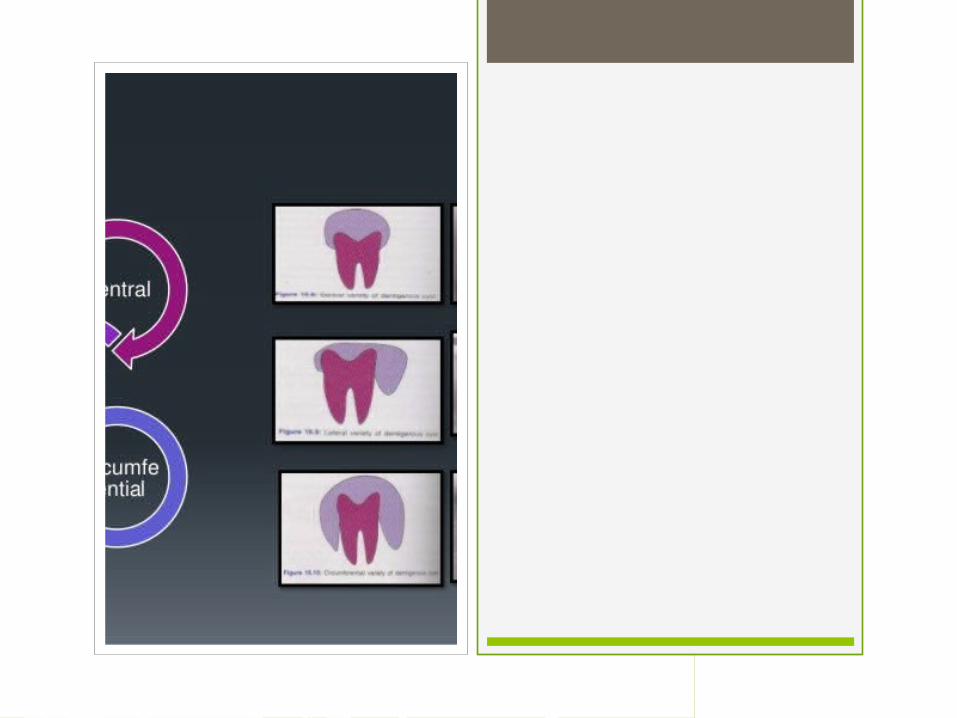
around the impacted tooth in three variation - 1.circumferential
2.lateral 3.coronal or central
HISTOLOGICAL FEATURE 1. The cystic lining composed of
reduced enamel epithelium 2. This epithelium may occasionally
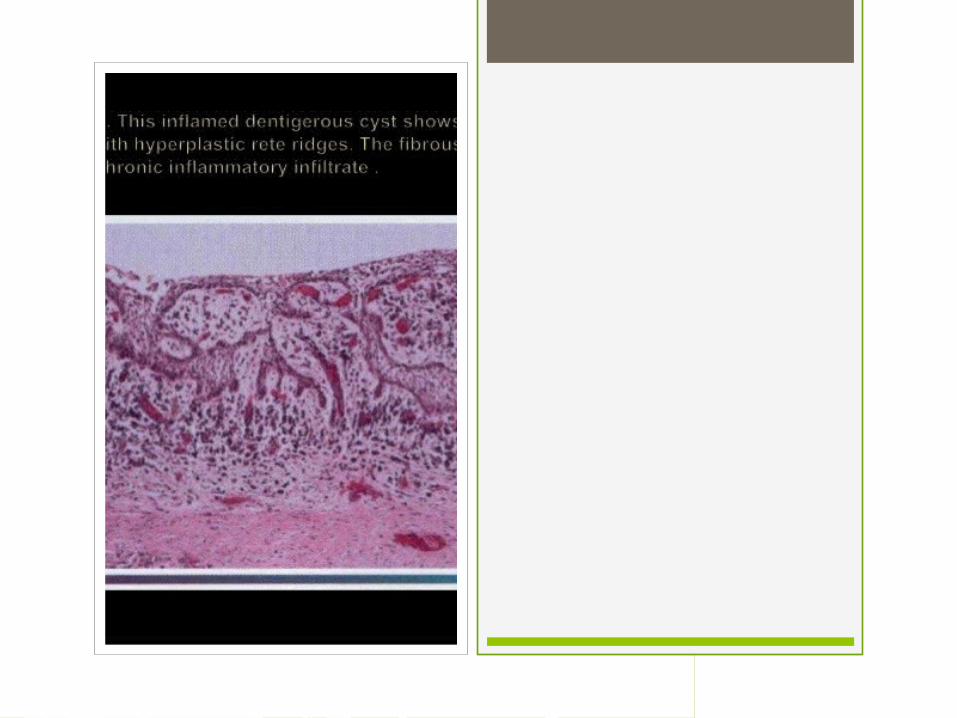
keratinize by metaplasia . 3. Chronic inflammatoryt cells may
found in case of 2ndary inflammation .
INVESTIGATION - 1. Orthopantomograph . 2. CT scan . 3. 3D CT scan . 4. Extra – oral radiograph – P/A .5. Lateral veiw of the mandible . 6. P/A veiw maxilla in water`s pasition .7. Incision biopsy . 8. Blood for TC,DC,ESR and HB%9. Blood for BT , CT . 10. Random blood glucose level . 11. HBs Ag .
TREATMENT - Dentigerous cyst can be treated in one of the following basic methods –
1. Enucleation . 2. Marsupialization . 3. A Staged Combination of the two
procedures . ( Enucleation after marsupialization 04. Enucleation with curettage .
ENUCLEATION - Instrument required –
Oral surgical set . Oral surgical drill with irrigation .
Positioning – Standard for the operating theatre .
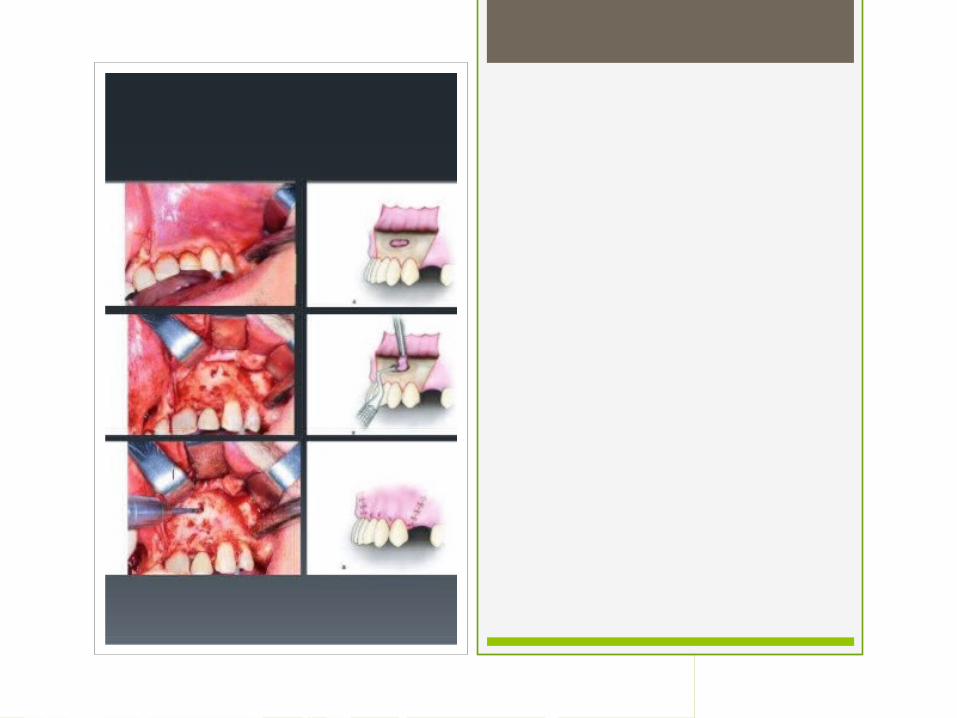
operative procedure Administration of local and general
anesthesia A soft tissue flap is outline and a single
layer mucoperiosteal flap is raised to expose the bone overlying the cyst
Bone is removed using a drill or chisel to gain access to the cyst cavity
The cyst lining is stripped from the wall of the cavity and retained for histological examination
The unerupted third molar is elevated from the cavity after further bone removed
The cyst cavity is thoroughly irrigate,any remnant of cyst lining removed,and the flap suture in its original position
The oral cavity and pharynx are inspected and cleared by suction ,and the throat pack removed
The tip are lubricated with petroleum jelly or steroid ointment
ADVANTAGE OF ENUCLEATION 1 Primary closer of the wound 2 Healing is rapid 3 Postoperative care is reduce 4 thorough examination of the entire
cystic lining can be done
DISADVANTAGE In young persone,the unerupted teeth
in dentigerous cyst will be removed with the lesion.
Removal of large cysts will weaken the mandible make it prone to jaw fracture.
3 damage to adjacent vaital structures 4 pulpal necrosis
ADVANTAGE OF MARSUPIALIZATION 1 Development of a thickend cystic
lining , which enucleation easire . 2 Spares adjacent vital structures. 3 Combined approach reduces
morbidity. 4 Accelerated healing process. 5 Allows histopathological examination
of residual tissue.

DISADVANTAGE Patient has to undergo secondary surery and the possible complicated that are involved with any surgery procedure
PROCEDURE OF MARSUPIALIZATION Administration of local anesthesia
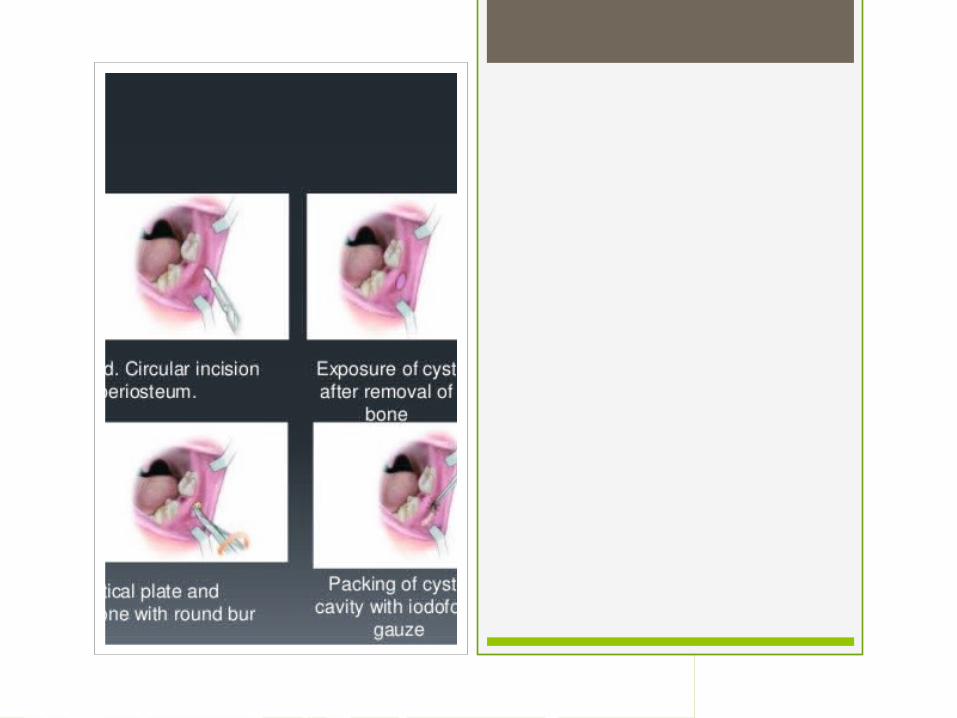
The incision ismade deep involving the mucoperiostom, bone and the cystic lining if the bone is thick it can be removed with chisel or dental bar.
Thereby cutting awindow in the roof of the cyst.
The fluid content of the cyst is evacuated by suction
The cystic lining is sutured with the oral mucosa around the opening.
The cystic cavity is picked with iodoform gauze loosely.
The cavity is irrigated and pack is changed every four – five day,ever time using a smaller pack than earlier
The cystic epithelial lining is transformed into normal mucous membrane.
Slowly the cavity fills up because of release of fluid pressure in the bone .Regeneration occurs beneath the defect.
If the bony cavity more than 2cm than reconstruction is done
CASE REPORT An 20 year old male patient presented
to the out patient department of Oral & Maxillofacial Surgery with a swelling in the maxillary anterior region , which was gradually incresing in size over the past two months.
H/O PRESENTING COMPLAINTS The patient states that he was
reasonably alright 2 months ago , then he developed a
swelling in the maxillary anterior region , which was gradually increasing in size over the past two months.
PAST HISTORY Nothing contributory FAMILY HISTORY All family members are in good health GENERAL EXAMINATION General examination, the patient was apparently healthy.
LOCAL EXAMINATION - 1.Extra oral examination A. Inspection
Facial symmetry – Bilaterally symmetrical Site – The maxillary anterior region Shape – oval Size – approximately 4cm Surface – normal Margin – well defined Colour -normal
B . Palpation – Swelling – Surface – smooth Tenderness – absent Consistency – firm Margin – well defiend Temperature – normal
INTRA – ORAL EXAMINATION Inspection –
Oral mucosa – Normal , pale pink in colour Tongue and frenum attachment – Normal & adequate
Gingiva – NormalDentition – A supernumerary tooth was observed lying horizontally within the lession,with distinct crown. Palpation: Nothing contributory

Investigation : OPG
TREATMENT Surgical enucleation of the cyst was
chosen as the treatment of choice

HEALING PROCEDURE AFTER BONE GRAFT
1. Osteogenesis – If there is osteoblast present I graf and if it is viable & help in new bone formation , the process is called osteogenesis . 2. Osteoinduction – If BMP helps in bone regenertion and accelerate bone healing process ,the process is called osteoinduction .
3 . Osteoconduction – If blood vessels present in graft invade surrounding & helps in remodelling of graf & formation of new bone , the process is called osteoconduction .
COMPLICATION -
1. Recurrence due to incomplete surgical removal .
2. Permanent bone deformation or pathological bone fracture .
3. Extensive bone destruction . 4. Loss of permanent tooth. 5. Development of squamous cell
carcinoma , mucoepidermoid carcinoma and ameloblastoma
REFERANCE 1. Text book of oral & maxillofacial surgery
neelima anil malik 2. Text book of oral & maxillofacial surgery S.M
Balaji. 3. Text book of oral & maxillofacial surgery Vinood kapoor 4.INTERNET: a.en.wikipedia.org b.mediscape.com
CONCLUSION - As dentigerous cysts are asymptomatic they can attain considerable size without the notice of the patient and this warrants they early clinical and radiographic detection of the cyst so that early treatment strategies will prevent or decrease the morbidity associated with the same .

![Case Report Orthokeratinized Odontogenic Cyst: A Report of … · 2019. 7. 31. · such as dentigerous cyst or paradental cyst [ , ]. Odon-togenic tumours such as ameloblastoma and](https://img.dokumen.tips/doc/110x75/614074aa1664f1518558c43e/case-report-orthokeratinized-odontogenic-cyst-a-report-of-2019-7-31-such-as.jpg)