Embed Size (px)
Citation preview

Ann. Hum. Genet., Lond. (1966), 29, 377 W i t h 5 plates Printed in Greut Britain
Hereditary brachydactyly
377
BY D. HOEFNAGEL AND P. S. GERALD Departments of Pediatrics and Pathology, Dartmouth Medical School, Department of Pediatrics,
Mary Hitchcock Memorial Hospital, Hanover, New Hampshire; Department of Pediatrics, Harvard Medical School, The Children’s Hospital Medical Center, and the Blood Grouping Laboratory of Boston, Nassachusetts
The term brachydactyly, used in the strict sense, refers to a congenital symmetric shortening of all fingers and toes. This shortening is caused by anomalies or absence of bony segments of the digits ; usually not all segments are involved simultaneously and minor anomalies of the other bones of hands and feet are frequently also present. The various types of brachydactyly can only be defined with radiography.
In 1905 Farabee described a particular form of brachydactyly in a kindred in which he recognized an autosomal dominant inheritance pattern for the trait ; this pedigree has recently been extended (Haws & McKusick, 1963). According to Farabee the shortness of the digits was caused by the congenital absence of the middle phalanx and he spoke of a ‘ hypophalangia, or a diminution in the number of phalanges ’. This interpretation was challenged by Drinkwaker (1907/8,1915), who described two similar brachydactylous kindreds in whom the brachydactgly of some fingers was due to synostosis of a rudimentary middle phalanx to the distal one, resulting in a total of two bony elements. Other reports of this particular form of brachydactyly include those of Iltis (1944) and Komai (1953); these authors refer to the condition as true or typical brachydactyly, conforming to type A, of Be11 (1951). In two other kindreds reported by Drink- water (1912,1913/14) the brachydactyly was caused by a rudimentary, but separately present, middle phalanx ; Drinkwater called this form ‘ minor-brachydactyly ’.
In the present study we record clinical, radiographic and genetic findings in a family with ‘true ’ brachydactyly ; observations on the dermatoglyphic patterns will be presented in an addendum by Prof. L. S. Penrose and Dr Sarah B. Holt.
INTRODUCTION
DESCRIPTION OF THE FINDINGS
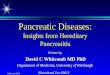
The brachydactyly of the propositus was noted when he was admitted to the hospital following a traumatic fracture of the right elbow. After the type of brachydactyly had been defined by radiography, other members of the family were studied (Text-fig. 1). The maternal grandmother of the propositus refused to co-operate in the studies, but she was reliably known to have brachydactyly of the type present in her daughters; the maternal grandfather had normal hands and feet. Complete clinical, radiographic, blood grouping and dermatoglyphic studies were obtained on the propositus, his parents and sibs ; the other members of the kindred only consented to study of their dermatoglyphs.
The hands and feet of the unaffected subjects were normal in every respect and they will not be described in detail, except for the dermatoglyphic findings. General health and mental status of the subjects examined were entirely normal. There were no abnormalities aside from those of the hands and feet, except for a relatively short stature of the affected subjects and discrepancy

378 D. HOEFNAGEL AND P. S. GERALD
Table 1. Metrica2 data Subject
pedigree number in Text-fig. I
11. I (N) 11.2 (B) 11. 3 (B) 11. 4 (N) 111. I (B) 111. 2 (N) 111. 3 (B) 111. 4 (N) 111. 5 (B) 111. 6 (N) 111. 7 (B) 111. 8 (B)
I
Age (years)
41 4' 39 44
8 5 3
I 2 I 0
8 6 4
Stature (in.)
61
71 51
39
55
669
64%
46
63
534 47Q 44*
Arm span (in.)
66 534 564 7 4
46
624 47%
41 B
44
35
53
39
B, Brachydactylous; N, unaffected.
Hereditary brach ydactyly kindred 25
9 Affected, not examined
7 r)' Affected 0 d N o t affected
Fig. 1
between standing height and arm span (Table 1). The brachydactylous hands and feet were broad and square with symmetrical shortening of all digits, particularly the fingers (Plates, figs. 1-20) ; the feet appeared to be less abnormal than the hands. The skin was coarse and loose, the palms were compressible by lateral pressure because of wide intermetacarpal spaces and the fingers were hyperextensible. The terminal phalanges of the third and fourth fingers were deviated toward each other and these fingers also showed a minor degree of volar flexion con- tracture (camptodactyly). Simian creases were present on the palms of several hands and each finger had a single skin-crease on the dorsal and volar aspect corresponding to the only inter- phalangeal joint present in each finger. The nails and sweating were normal and the trait did not cause significant functional disability, but it was difficult to make a complete fist.
Radiographs of hands and feet disclosed a large number of anomalies (Plates, figs. 1-20). All bones were small, but the brachydactyly was primarily due to smallness and abnormalities of the bones of the digits. In the toes this shortness was due to absence of the middle phalanx

Hereditary brach ydact yl y 379
of toes 11-V and shortness of the first metatarsal and proximal phalanx of the first toe. The metatarsal bones appeared less abnormal than the metacarpal ones. The middle phalanges in the hands showed a spectrum of anomalies. In some fingers a hypoplastic middle phalanx was present as a separate segment (fingers I11 of 11. 3) and in others the middle phalanx had been incorporated in the distal one (finger IV, right hand of 11. 3). In fhgers with two bony elements, it could only be surmised that fusion had taken place between the middle and distal phalanx (fingers I1 and V of 11. 3). There was no difference clinically between a finger with a separate rudimentary middle phalanx and one with two phalanges; both types had only one inter- phalangeal joint and there was no difference in length of the fingers. The proximal phalanx: of the first finger was short and often malformed. In the hands of the children several phalangeal epiphyses were absent. The metacarpal bones were short, widely spaced, had flat distal articular surfaces and frequently showed accessory epiphyses.
A short-term culture of the peripheral blood of the propositus and of that of his mother showed normal numbers of chromosomes and normal karyotypes. The results of the blood grouping studies are shown in the Appendix.
DISCUSS I0 N
The clinical and radiographic findings in the brachydactylous subjects conform in general to those described by Farabee (1905), Drinkwater (1907/8, 1915), Iltis (1944) and Komai (1953). The condition shows interfamilial as well as intrafamilial variation; in the present family it is not possible to judge how closely the radiographs of the hands of the children, after closure of the epiphyses, will resemble those of the mother. It is planned to obtain serial radiographs of the hands in order to ascertain the pattern of growth and development of the bones of t,he fingers. This could also be helpful in confirming or refuting Drinkwater's (1907) observation that, in the fingers with two bony elements after epiphysial closure, there has not been a con- genital absence of the whole middle phalanx, but fusion of a rudimentary middle phalanx h.as occurred with the distal phalanx. Drinkwater based this interpretation on the cubical shape of the base of the terminal phalanx in carriers of the trait, which resembled the shape of the middle phalanx in those fingers in which a separate rudimentary middle phalanx was present ; normally the base of the terminal phalanx is triangular or pyramidal in shape. Another interpretation, however, is that the structure which resembles a rudimentary middle phalanx is in fact the epiphysis of the distal phalanx, which has acquired an unusual shape because of the complete absence of the middle phalanx and its epiphysis. The growth centre of the distal epiphysis is therefore located where normally the diaphysis of the middle phalanx is found.
Table 2. Lod scores
Recombination fraction Blood-group Scoring r A >
locus method* 0.05 0'10 0'20 0.30 0.40
ABO 2 2 + dz +0'149 +0-125 + 0'079 + 0.038 +o.oro MNSs 2, - 1'442 - 0.887 - 0.388 -0.151 - 0.036
DuffY 2 2 + dz - 0.785 - 0'494 - 0'222 - 0.088 - 0'02 I Rhesust 2, +el - 1'456 - 0.899 - 0.396 -0.156 - 0.037
* Morton, N. E. (1955). t The mother (11. 3) is assumed to be D/D" and the children D/d (positive reactors) or D"/d (wecik
reactors).

380 D. HOEFNAGEL AND P. S. GERALD
Blood grouping studies were performed on 11. 3 and 11. 4 and their five children (Appendix). Information was obtained regarding possible linkage with the ABO, MNSs, Rhesus and Duffy blood group loci (Table 2). The quantity of data is insufficient for linkage or non-linkage of these blood group loci with the hereditary brachydactyly locus to be demonstrated.
In the kindreds with this form of brachydactyly, the trait is inherited in an autosomal dominant manner. There is no record of a marriage of two affected individuals. Blood grouping studies in kindreds with this trait have hitherto not been reported.
SUMMARY
An account is given of a family with hereditary brachydactyly of the type described by Farabee. Blood grouping studies in one branch of the kindred did not demonstrate either linkage or non-linkage between the hereditary brachydactyly locus and the ABO, MNSs, Rhesus and Uuffy blood group loci.
IVe wish to thank Dr Stuart W. Russell, Orthopedic Department, Hitchcock Clinic, for permission to study this kindred; Dr John Bargoot for help in reading of the radiographs; Mr Wayne C. Stiller and Miss Mary Spencer of the Medical Illustration Department, Mary Hitchcock Memorial Hospital, for photographic assistance ; Miss Helen Moulton and Miss Elaine Feingold of the Blood Grouping Laboratory for special blood grouping tests; and Mr William Bucknall and Miss Helen Moulton of the Blood Grouping Laboratory for the linkage calculations.
This work was supported by grants (GM 10210 and GM 09107) of the United States Public Health Service and a grant of the Charles H. Hood Dairy Foundation.
REFERENCES
BELL, J. (1951). On hereditary digital anomalies. Part I. On brachydactyly and symphalangism. Treas. Hum.
DRINXWATER, H. (190718). An account of a brachydactylous family. Proc. Roy. SOC. Edinb. 28, 35-57. DRINKWATER, H. (1912). Account of a family showing minor-brachydactyly. J . Cienet. 2, 21-40. DRINKWATER, H. (1913/14). Minor-brachydactyly. No. 2. J. Genet. 3, 217-20. DRINKWATER, H. (1915). A second brachydactylous family. J. Genet. 4, 323-39. FARABEE, W. C. (1905). Inheritance of digital malformations in man. P a p . Peabody M u . 3, 69-77. HAWS, D. V. & MCKUSICK, V. A. (1963). Farabee’s brachydactylous kindred revisited. BUZZ. J. HopkinsHosp.
ILTIB, H. (1944). A now case of typical brachydactyly. J. Hered. 35, 1 4 6 8 . KOMAI, T. (1953). Three Japanese pedigrees of typical brachydactyly. J. Hered. 44, 79-85. MORTON, N. E. (1955). Sequential tests for the detection of linkage. Amer. J. Hum. Genet. 7 , 277-318.
Inherit. 5 , 1-31.
113, 20-30.

L4nn,al~ qf Humun Genetics, Vol. 29, Part 4
D. HOEFNAGEL AND P. S. GEltAlL)
Plate 1

Annuls of Humrut Genet ics, Vol . 29, Part 4 Plate 2

Annals of Human Genetics, Vol. 29, Part 4
D. HOEFNAGEL AND P. S. GERALD
Plate 3

Plate 4
1). IlOIIFSXGEL ASD 1’. S . GERALD

Annals of Human Genetics, Vol. 29, Part 4
D. HOEFNAGEL AND P. S. GERALD
Plate 5


Hereditary brachydactyly 38 1
APPENDIX Pedigree no.
Sex Disease
H A B D C E
A1
C
0
f G
Se* Le* M N S
Pl
8
FY" Jk" Jkb Gm' Gmb Gm"
11. 3
F + + + + +
0
0
0 0
+ + + + + + + + + + +
0
0
0
0
0
11.4
M 0
+ + 0
0 0 0
0 + + + + + + + + + + + + +
0
0
0
0
- 3
111.4 111. 5 111.6 111.7 111. 8 F M F M M 0 + 0 + + + + 0 + + 0 0 + 0 0 + + 0 + + 0 + + + + + +
0
0 W + 3. + + +
0
0 W + + + + +
0
0 W + + + + +
0
0
+ + + + + +
0
0 0 0 0 0 + + + + + + + + + + 0 + + 0 0 + + + + + 0 + + 0 0 + + + + + 0 + + 0 + + 0 0 0 0 + + + + + + 0 + + + + + + + + 0 0 0 0 0
+ , Positive reaction; 0, negative reaction; W, weak reaction. * Se + = ABH substance present in saliva; Le + = Le; substance present in saliva; Le o = Lea sub-
All persons were tested for the factors Mt', Vw, Mg, Lu", Inv.', He, S<, Ra", V, C", Wr", Be and were
All persons were tested and found to be: K; - I , -3 , 4; Hp 2-2; Tf c-c. All persons were tested for the factors Xg", I, Ge, U and were positive.
stance not detected in saliva.
negative.
EXPLANATION OF PLATES
PLATE 1
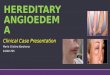
Figs. 1 , 2. Male 111. 5 (Text-fig. 1). Chronological age 10 years 2 months. Left hand showing brachydactyly, simian crease on palm and single skin fold on dorsal and volar surfaces of fingers 11-V. The right hand was similarly affected, but could not be photographed because the right arm was in an orthopaedic cast. Fig. 3. Male, 111. 5. The brachydactyly is on clinical inspection not as evident in the feet as in the handls.
PLATE 2
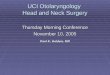
Fig. 4. Male 111. 5. Radiograph of left hand. Bone age between 8 and 9 years. The carpal bones are smdl, particularly the lunate. The f is t metacarpal is malformed and has an accessory distal epiphysis; the secmd metacarpal has an accessory proximal epiphysis. The proximal phalanx of the thumb is underdeveloped and lacks an epiphysis. The rudimentary middle phalanx of the second finger is fusing with the distal one; neither bone has an epiphysis. In the third finger the epiphysis of the proximal phalanx is malformed and fusing; the rudimentary middle phalanx is fusing with the distal one. The fourth finger has a rudimentary middle phalanx and a malformed proximal one, which lacks an epiphysis. The fifth h g e r has a short, stubby proximal phalanx, which lacks an epiphysis; the middle phalanx is fusing with the distal phalanx or is absent and the structure between the diaphyses of proximal and distal phalanges is the epiphysis of the distal phalanx (see discussion).

D. HOEFNAGEL AND P. S. GERALD Fig. 5. Male 111. 5. Radiographs of feet. The following changes occur bilaterally. There is an overdeveloped proximal epiphysis of the distal phalanx of the first toe with underdevelopment of the proximal phalanx. The middle phalanges of toes 11-V are absent; there is notching of the terminal phalanges of these toes.
Figs. 6 and 7. Female 11. 3 (Text-fig. 1). Chronological age 39 years. The hands show brachydactyly, simian creases on palms, single skin creases on dorsal and volar surfaces of fingers 11-V. The middle and ring fingers are deviated toward each other and there is a mild degree of camptodactyly (volar bending) of the fourth fingers. Fig. 8. Female 11.3. The space between first and second toes was broader than shown in the photograph. The right fourth toe was very small and hyperextensible.
PLATE 3
Fig. 9. Female 11. 3. Radiographs of the hands. The proximal phalanges of the thumbs are small. The second and fifth fingers lack a middlo phalanx and both third fingers have a small middle phalanx. There is a rudi- mentary middle phalanx of the left fourth finger, which in the right fourth finger is fused with the distal phalanx. Themetacarpals are more widely spaced than usual; the styloid process of the ulna is absent. The distal phalanges of the fourth fmgers are radially deviated. The distal articular surfaces of some metacarpals are flat. Fig. 10. Female 11. 3. Radiographs of feet. The fourth metatarsal on the right is shortened. In the f i s t toe the proximal and distal phalanges are fused; in the third, fourth and fifth toes the proximal phalanges are shortened. The middle phalanges of the toes 11-V are absent. Figs. 11, 12. Male 111. 7 (Text-fig. 1). Chronological age 5 years 8 months. The hands show brachydactyly, simian palmar creases, single creases on the doreal and volar surfaces of fmgers 11-V, deviation toward each other and camptodactyly of fingers I11 and IV. Fig. 13. Male 111. 7. The feet show brachydactyly and broad spacing between the first and second toes.
PLATE 4
Fig. 14. Male 111. 7. Radiographs of hands. Bone age approximately 4+ years, but ossification centre of the Iunate bone is absent. The first metacarpals are spatulate and have an accessory distal epiphysis. The proximal phalanx of the thumb is underdeveloped. There is an accessory proximal epiphysis of the second metacarpal. The proximal phalanges of the first and fifth finger are shortened and the proximal phalanx of the fourth finger lacks an epiphysis. The distal phalanges of the second and fifth digits lack an epiphysis and in these fingers the middle phalanx is rudimentary and lacks an epiphysis. The third and fourth fingers have small middle phalanges without epiphyses.
Fig. 15. Male 111. 7. Radiographs of feet. The first metatarsal and the proximal phalanges of the first, third, fourth and fifth toes are shortened. Middle phalanges are absent in toes 11-V. Figs. 16, 17. Male 111. 8 (Text-fig. 1). Chronological age 4 years 3 months. The hands show brachydactyly and single creases on the dorsal and volar surfaccs of fingers 11-V. The third and fourth fingers deviate toward each other and also show camptodactyly. Fig. 18. Male 111. 8. The feet show brachydactyly and a marked degree of spacing between the first and second toes.
PLATE 5
Fig. 19. Male 111. 8. Radiographs of hands. Bone age 3 years 3 months; the lunate bone is not ossified. The following changes are bilateral. The proximal phalanx of the thumb is short. The middle phalanges of fingers 11-V are rudimentary and lack epiphyses. The distal phalanges of fingers I1 and V lack an epiphysis. Fig. 20. Male 111. 8. Radiographs of feet. The proximal phalanx of the first toe is shortened and the middle phalanges of toes 11-V are absent.