Embed Size (px)
Citation preview

7 2 2 Editorial correspondence The Journal of Pediatrics May 1996
Table. Clinical data on CF pat ients carrying the T338I mutat ion
Maternal Paternal Sweat Patient chromosome Maternal chromosome Paternal Age chloride ion Initial Pseudomonas
No. Sex mutation ancestry mutation ancestry (yr) (mmol/L) symptoms aeruginosa
1 F T3381 Sardinia R117H Northern Italy 12 50 Hypochloremic alkalosis - 2 F T3381 Sardinia R1158X Sardinia 10 98.6 Bronchopulmonary pneumonia - 3 F T338I Sardinia R1158X Sardinia 8 80.25 Asymptomatic CF 4 M T3381 Sardinia DF508 Northern Italy 30 98 Allergic bronchopulmonary +
aspergillosis; Pseudomonas infection; nasal polyposis; bronchiectasis
Patients 2 and 3 are sisters•
cystic fibrosis transmembrane regulator (CFTR) gene either in the homozygous or in the heterozygous state. We report our experience on a further four patients with CF who carry the same mutation, be- cause this additional information can increase our understanding of genotype-phenotype correlations. Among patients with CF who are followed at the Milan CF center, all studied at the molecular level, we found T338I missense mutation in 3 (0.37%) of 812 chromo- somes (two of the three patients are sisters). 2 Clinical data on our patients are shown in the Table.
All the patients have pancreatic sufficiency, identified by normal fecal fat balance (i.e., 3 days of fecal collection to evaluate the ab- sorption coefficient2), with normal growth. Patients 1 and 2, iden- tified in the first year of life, and patient 3, identified by prenatal diagnosis, by restriction fragment length polymorphism (the parents decided to continue the pregnancy), have no pulmonary disease and have a normal life. In the neonatal period, immunoreactive trypsin test results for patients 2 and 3 were below the 99th percentile. Pa- tient 4, identified in adult life (at 27 years 3 months of age), has at present a moderate pulmonary involvement (Pseudomonas chronic lung infection, chest x-ray score by Chrispin and Norman equal to 18, forced vital capacity 97%, and forced expiratory volume in 1 second 75% of the predicted value), and he has azoospermia. He has a normal social life and married in 1995.
The patient in whom hypochloremic metabolic alkalosis was di- agnosed is the only one with borderline chloride values on repeated sweat test; this finding may be explained by the presence of the R117H mutation on paternal chromosome. It is well known that missense mutation R117H is associated with a low chloride sweat concentration) This female patient had symptoms during an extraordinarily warm and arid summer in Milan. The pathogenesis of hypocloremic alkalosis in the first year of life (also in patients with CF whose chloride sweat concentration is low) may be due to a low intake in chloride and sodium provided by the infant diet.
Our data confirm the data presented by Leoni et at.: T3381 mis- sense mutation could be considered a mild mutation conferring both pancreatic sufficiency and mild pulmonary phenotype, Further- more, in our series T3381 was detected only on CF chromosomes of patients of Sardinian ancestry. Our data, together with the data of Leoni et al., allow us to give more appropriate and precise ge- netic counseling to families carrying this mutation. Knowing a pa- tient' s regional ancestry could be helpful in mutation analysis of CF chromosomes.
Rita Padoan, MD Manuela Seia
Laboratorio di Ricerche Cliniche. Istituti Clinici di
P e rf e zionament o
Laura Cremonesi
IRCCS H.S. Raffaele, D1BIT, Unitd di Genetica
Annamaria Giunta, MD Centro di Riferimento Regionale per la Fibrosi Cistica della
Regione Lombardia Universitd degli Studi di Milano
Milan, Italy 9/35/72152
R E F E R E N C E S
1. Leoni GB, Pitzalis S, Podda R, et al. A specific cystic fibrosis mutation (T3381) associated with the phenotype of isolated hypotonic dehydration. J Pediatr 1995; 127:281-3.
2. Brancolini V, Cremonesi L, Belloni E, et al. Search for muta- tions in pancreatic-sufficient cystic fibrosis Italian patients: de- tection of 90% of molecular defects and identification of three novel mutations. Hum Genet 1995;96:312-8.
3. Cystic Fibrosis Genotype-Pbenotype Consortium. Correlation between genotype-phenotype in patients with cystic fibrosis. N Engl J Med 1993;329:1308-13.
Enteropathy and IgG subclass deficiency To the Editor:
I read with special interest the article by Smith et al. 1 regarding familial enteropathy with villous edema and IgG2 subclass defi- ciency. The disease is characterized by acute episodes of intermit- tent life-threatening secretory diarrhea, and the authors postulated "that a nonspecific infectious trigger precipitates the secretory di- arrhea, in the presence of an abnormal intestinal mucosa and a re- duction of IgG2 subclass antibody." They further stated that "some children with the syndrome had low total IgG values in the asymp- tomatic phase, and all but one patient had IgG2 subclass deficiency but without recurrent upper respiratory tract infections."

The Journal of Pediatrics Editorial correspondence 7 2 3 Volume 128, Number 5, Part 1
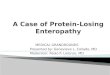
Table. Serum immunog lobu l ins and IgG subclasses in four chi ldren wi th prote in- los ing enteropathy
Patient Age Total No, Diagnosis (yr) IgM IgA IgG IgG I IgG2 IgG3 IgG4
1 CMV-induced M6n6trier's 1 ~ 65 59 390 300 20* 45 2.5 disease
2 CMV-induced M6n6trier's 2 71 41 260* 225 O* 12 2.0 disease
3 Idiopathic protein-losing 13 92 18" 432* 264* 78* 32 2.0 enteropathy
4 Protein-losing enteropathy 16 37* 28* 245* 172" O* 36 5.0 caused by fight-sided 17 86 28* 374* 269* 5* 54 10.0 heart failure (examined twice)
The lgG subclasses and total IgG were measured by nephelometry. All results are expressed in milligrams per deciliter. CMV, Cytomegalovirus. *Below the normal range for age in our laboratory.
It is unlikely that the 13 patients tested in the asymptomatic phase of the disease had a specific deficit of IgG2 production. More than 50% of the affected children also had low total IgG values, a find- ing that usually cannot be explained by low IgG2 levels alone be- cause IgG2 comprises only 25% to 30% of the total lgG. 2 In addi- tion, the authors mentioned that some affected individuals also had low serum IgG1 and lgG3 values.
These patients may have had a deficit in the intestinal mucosa, causing continuous low-grade loss of immunoglobulins through the intestinal lumen, rather than a primary deficit in the humoral immune system, as suggested by the authors. A loss of immuno- globulins through the digestive system may occur in patients with protein-losing enteropathy; these losses may be limited in some IgG subclasses and more pronounced in others because of the different physical and chemical properties of these proteins. 2 Testing IgG subclasses in protein-losing enteropathy may result in different profiles of IgG subclasses with a prominent low level of IgG2, as shown in the four children followed by me in recent years (Table).
B. Z. Gar~., MD Kipper hlstitute of Pediatric Immunology
Schneider Children's Medical Center of Israel Beilinson Medical Campus Petah Tiqva 49202, Israel
9/35/72153
R E F E R E N C E S
1. Smith LJ, Szymanski W, Foulston C, Jewell LD, Pabst HF. Familial enteropathy with villous edema and immunoglobulin G2 subclass deficiency. J Pediatr 1994:125:541-8.
2. Schur PH. IgG subclasses: a review. Ann Allergy 1987;58:89-100.
Hypotonic dehydration in cystic fibrosis: Mild or severe disease phenoNpe? To the Editor.
Eight Sardinian children, seen because of isolated hypotonic de- hydration, mostly chloride deficiency metabolic alkalosis, were re-
cently found to have the cystic mutation T3381 by Leoni et al. 1 The mentioned patients likely have a very mild cystic fibrosis pheno- type, because none had pulmonary or pancreatic involvement. These exciting observations might unfortunately lead one to assume a mild phenotype in all patients with cystic fibrosis and a tendency toward hypotonic dehydration.
Hypotonic dehydration is a rather common, often unrecognized complication of cystic fibrosis even in a temperate climate. 2-4 Data from the literature and our own experience indicate that the men- tioned complication occurs especially in patients aged less than 2 years, in patients with severe exocrine pancreatic insufficiency, and in patients with severe pulmonary involvement early in life. 2"4
It is therefore tempting to conclude that in patients with cystic fi- brosis and both pulmonary and pancreatic involvement, hypotonic dehydration indicates a severe cystic fibrosis phenotype. On the contrary, the disease phenotype might well be benign in children with isolated hypotonic dehydration, such as those reported by Le- oni et al.
Mario G. Bianchetti, MD Simonetta Mauri. MD
University Children's Hospital lnsel~pital
3010 Berne, Switzerland 9/35/72154
R E F E R E N C E S
1. Leoni GB, Pitzalis S, Podda R, Zanda M, Silvetti M, Caocci L. et al. A specific cystic fibrosis mutation (T338I) associated with the phenotype of isolated hypotonic dehydration. J Pediatr 1995;127:281-3.
2. B6rard E, Maillotte AM, Albertini M, Delalandre E, Boutt6 P, Mariani R. Mucoviscidose rtv616e apr~s une dtshydratation avec alcalose hypochloronatrtmique chez trois nourrissons et un nouveau-nt. Arch P6diatr 1994:1:42-5.
3. Soio A, Rodriguez-Soriano J, Vitoria JC, Vazquez C, Villate A. Chloride deficiency as a presentation or complication of cystic fibrosis. Eur J Pediatr 1994;153:825-8.
4. Pedroli GL, Liechti-Gallati S, Mauri S, Birrer P, Kraemer R, Foletti-Jtiggi C, et al. Chronic metabolic alkalosis: not uncom- mon in young children with severe cystic fibrosis. Am J Neph- rol 1995;15:245-50.